History
Enophthalmos may be sudden, static, non-changing (as may occur with trauma), or progressive. Sudden appreciation of enophthalmos does not necessarily imply sudden development. Depending on the cause, enophthalmos may progress over any time frame, ranging from minutes to years. Most causes of enophthalmos are progressive, including trauma and congenital deformities, because inflammation and swelling immediately after trauma may prevent achievement of the total final degree of enophthalmos, and congenital enophthalmos may progress as certain parts of the face continue to develop while others do not.
Physical
Mild degrees of bilateral enophthalmos may be difficult to determine without radiographic studies or old photographs for comparison, but unilateral enophthalmos often is obvious when comparing one eye with the other. Specific changes include the following:
-
Narrowed vertical eyelid fissure (vertical fissure may be widened or normal if associated with downward displacement of the eye, also known as hypoglobus or globe ptosis)
-
Superior sulcus deformity (deepened upper eyelid crease)
-
Lost fullness of fat bulge in upper and lower eyelids
-
Can be associated with hypoglobus (downward displaced eye), usually without significant associated diplopia (double vision) [6]
-
Other physical findings, depending on etiology
- Skin and eyelids
- Thinned skin, muscle, fat, or even bone in a linear array may suggest Parry-Romberg syndrome or linear scleroderma.
- Thickened indurated skin may suggest metastatic scirrhous carcinoma.
- Blue, boggy skin might indicate associated vascular malformation with varix.
- Fifth nerve function
- Decreased function of second division may suggest nerve entrapment in fracture.
- Decreased function of either of the first 2 divisions may suggest tumor infiltration or cavernous sinus involvement.
- Exophthalmometry measurement: This is important to establish progression or stability.
- Ocular motility: Dysmotility might suggest a mass (orbital tumor) or restrictive process (fracture).
- Skin and eyelids
Causes
Causes of secondary enophthalmos include the following:
-
Postnatal, inadequate, orbital cavity development
- Bone growth arrest (eg, ionizing radiation for retinoblastoma)
- Inadequate local tissue stimulation of orbital bone growth
- Intraorbital (eg, phthisis bulbi, anophthalmos, fat atrophy in childhood)
- Extraorbital (eg, maxillary bone growth problems)
-
Orbital cavity expansion
- Outward fracture of orbital bones: In order of frequency, fracture sites are as follows: floor, medial wall, lateral wall, and roof.
- Surgical expansion of the orbit (as in orbital decompression or expansion for thyroid orbitopathy)
- Silent sinus syndrome (ie, spontaneous, asymptomatic collapse of the maxillary sinus and orbital floor associated with negative sinus pressures)
- Orbital varix with presumed slow bone erosion when the varix fills during recumbent position
-
Volumetric loss of orbital contents
- Orbital fat atrophy
- Following concussive trauma
- Following severe inflammation or infection
- Following external beam irradiation
- Associated with wasting disorders (eg, Parry-Romberg hemifacial atrophy, linear scleroderma)
- Associated with nucleoside reverse-transcriptase inhibitors in HIV treatment [7]
- Contraction of orbital fat - Scirrhous carcinomas (most commonly metastatic breast, but pulmonary, prostate, and GI cancers may cause fat and globe retraction as well) [8]
- Following surgery (as in resection of a mass lesion associated with local fat atrophy)
- Phthisis bulbi or prephthisis bulbi
- Orbital fat atrophy
-
Pseudoenophthalmos
- Unilateral blepharoptosis
- Horner syndrome
- Contralateral exophthalmos
- Contralateral pseudoexophthalmos
- Contralateral high myopia
- Contralateral buphthalmos or megaloglobus
- Contralateral eyelid retraction
Physical Examination
The degree of enophthalmos is often appreciated and measured using an exophthalmometer, of which several varieties are available. Exophthalmometer measurements are highly position– and applied pressure–dependent, and the reliability of measurements, especially as performed by different examiners, may be low.
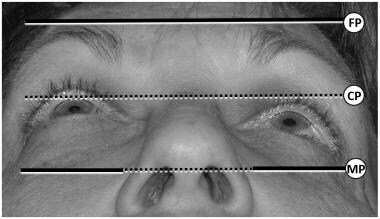
"Worms' eye" photographs, such as that shown in the image below, can be very helpful in documenting and monitoring enophthalmos. The photographs are taken at a standardized angle of head tilt, for example placing the tragus of the ear and the projection of the chin in a line parallel to the floor. An assessment of the anterior corneal projection, marked "CP" below, may be compared to the frontal process projection "FP" and the maxillary process projection "MP." In this photograph, the left eye is enophthalmic. If the lateral orbital rim is posteriorly displaced or the maxilla is hypoplastic or in-fractured, the more common exophthalmometers will provide inaccurate measurements.
Complications
Long-standing enophthalmos, especially associated with very extensive orbital trauma, may be associated with severe orbital scarring, and correction can be very difficult or impossible.
Complications of enophthalmos are mostly aesthetic, but certain problems may be associated with a posterior position of the eye, including the following:
-
Upper eyelid ptosis and lower eyelid reverse ptosis
-
Upper eyelid retraction if the enophthalmos is due to cicatricial problems or associated with hypoglobus, downward displacement of the eye
-
Ocular dysmotility and diplopia due to abnormal vectors induced upon the oblique muscles
-
Upper eyelid "standoff" from the globe with inadequate blink-induced lubrication if the eye lies posterior to the Whitnall ligament
-
Ocular surface irritation and drying due to air spaces at the lateral and medial canthi, where the eyelids remain attached to the orbital rim, but the globe is much more posterior.
-
Diminished visual field due to the relative prominent projection of the brow, lateral orbital rim, cheek, and nose
-
Enlarged tear lakes with inadequate tear mobilization down the lacrimal system and resulting vision blur and epiphora
Other complications may be associated with the development of enophthalmos, but not caused by the enophthalmos. Examples might include other facial trauma or systemic malignancy.
-
Eye and orbit.
-
Conventional frontal tomograph of a blow-out fracture.
-
Relative enophthalmos.
-
Enophthalmos.
-
Coronal computed tomograph of silent sinus syndrome.
-
Worms' eye view showing left enophthalmos.